The interview was conducted by Professor Daniel Gygax, leader of the SATW technologies for precision medicine topical platform.
Gideon Hönger and I are on a first-name basis. I was head of the degree programme when you started the part-time Molecular Life Sciences course at the FHNW. You worked as a research assistant in the Department of Biomedicine at the Centre for Teaching and Research at the University Hospital Basel. As a professor of bioanalytics, I was able to accompany you in your project work and on your path from bachelor's degree to doctorate. The few references I have made to your professional career suggest that you have gone your own way. Can you briefly describe this path for us?
Yes, first I was a pharmacobiology laboratory technician, then a primary school teacher and then an HIV test developer in the diagnostics department at Hoffmann-La Roche, before I found the job of a lifetime in the Department of Transplantation Immunology at the University Hospital Basel... I was extremely interested in the topic of organ compatibility/incompatibility, native/foreign, similar/dissimilar. I was able to take the further development of immunological tests in the context of transplantation into my own hands. It was an extremely exciting time, combined with professional stays in Canada and the USA and the establishment and in some cases Switzerland-wide standardisation of new tests for a more precise assessment of the immunological risk for kidney recipients. In order to gain a deeper understanding of the topics entrusted to me and to carry out my tasks more professionally, I began to study at the same time as working, first at the School of Life Sciences at the University of Applied Sciences Northwestern Switzerland in Muttenz, then at the University of Basel.
I read that the transplantation of an organ from a donor to a recipient is an extremely multifaceted process that gives patients with end-stage organ failure a second chance at life. There are probably important questions that need to be clarified at the beginning of a transplant.
In fact, it is particularly important to allocate a donor organ to the best possible recipient from an immunological point of view, which is only possible through meticulous diagnostic pre-tests and their correct interpretation. And that's exactly what I'm responsible for.
Why is this so-called molecular match between the body tissue of the organ recipient and the foreign organ of the donor so important?
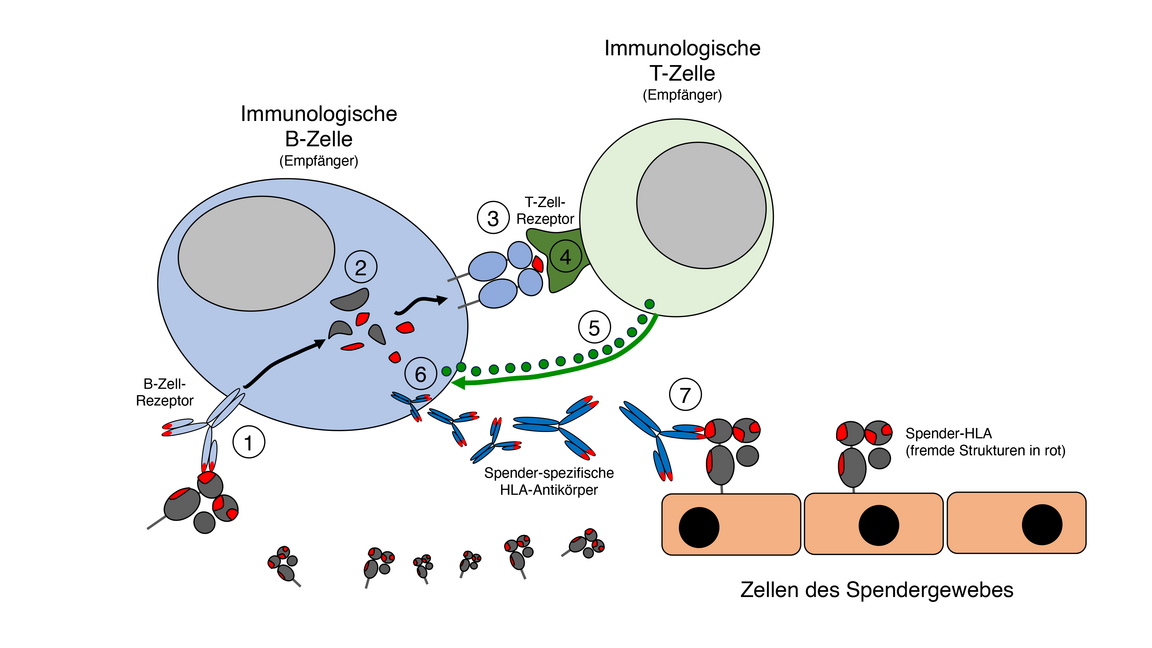
Our immune system is specialised in detecting and eliminating parasites. Every cell in the body has an alarm system that tells the circulating immune cells whether the proteins in the cell or its environment are endogenous or foreign. How does it do this? The alarm system continuously fragments proteins from the environment or the inside of the cell and presents parts of them - peptides - on so-called HLA molecules, which are located on the cell membrane. There they are continuously scanned by the receptors of specialised immune cells (T cells). If a receptor recognises a foreign peptide, the body cell in question is either destroyed or antibodies are formed against it. The strength of the alarm system is that many different peptides can be presented and recognised, which is why we are rarely ill. In order to be able to present many different peptides, we have several HLA molecule types, which differ from person to person. This is why we can survive as a whole population. However, in a transplant, this super-important system is - immunologically speaking - the main problem: the HLA molecules of the donor are also proteins, so they are also fragmented and presented as peptides on HLA molecules of the organ recipient. As a result, the patient's immune cells recognise them as foreign to the body - after all, they are structurally different - and attack them, in particular using donor-specific antibodies formed by type B immune cells (see image). Unfortunately, this leads to the destruction of the donor tissue and rejection of the transplant. A transplantation without simultaneously taking medication that suppresses the immune system is therefore unthinkable, unless the donor is an identical twin.
What is the secret of the distinction between the body's own and foreign peptides by the immune cells?
In the bone marrow, as well as in the thymus gland, immune cells learn very early in our development what is the body's own and what is foreign: all proteins present in the body are bound as peptides to the body's own HLA molecules and "shown" to the young immune cells: each immune cell checks whether its specific scanner, namely the cell's own receptor, can recognise structural components of the body's own proteins. In those where this is the case, something amazing happens: they voluntarily commit suicide! However, this makes perfect sense: it ensures that the immune system does not attack its own body! Only cells that have a specific receptor against potentially foreign proteins survive. Many billions of different receptors are needed to cover all possible foreign protein structures. This is why a whole army of immune cells is produced in this early developmental phase; each cell clone is equipped with a different receptor. Some of these will later save our lives because they have exactly the right receptor, which - to give an example - recognises the viral peptide presented on an HLA molecule and kills the virus-infected cell.
Can you explain to us how exactly HLA peptides of the donor differ from those of the recipient and is there a correlation between the number of different HLA structures and the probability of organ rejection?
In fact, individual HLA proteins differ greatly in terms of their amino acid composition, their three-dimensional structure and the peptides that can be presented. The number of these differences between donor and recipient HLA clearly correlates with the risk of immunological rejection. However, not every difference is of equal value. One of the topics in which I am involved in research is the characterisation of specific HLA differences in terms of their clinical risk level in the context of transplantation. The central question here is which differences can be "detected" at all, as certain peptides can be chemically loaded more or less well onto corresponding recipient HLA molecules.
Can you give us an overview of the methods used to determine the accuracy of fit of a donor organ at the cell and molecule level?
We use three methods in particular. To typify the aforementioned HLA molecules, we analyse the HLA genes using a high-resolution sequencing method (NGS), the result of which, the genetic code of the HLA genes, we translate into the HLA protein structure. The test is carried out on both the recipient and the donor and we then determine the differences.
A second method is used to search for HLA antibodies. We have to prevent other HLA structures from re-entering the body through the transplant, against which the recipient's body has already formed immunological memory cells. These can arise after pregnancies, transfusions or previous transplants. To do this, we incubate the recipient's serum with a set of artificial beads containing the 200 most common HLA molecules. If antibodies are present, they bind to the corresponding structures and it becomes clear whether they are donor-specific.
Finally, we simulate the transplantation in a test tube using a so-called cross-test. Here we use the actual donor cells that we obtain from the blood. We mix these with recipient serum and measure whether and how many antibodies recognise donor HLA molecule structures. This test should be negative.
Our conversation so far has centred on the molecular aspects that play an important role in organ transplantation. You gave us an insight into the complex immunological relationships and showed us that understanding these relationships is a prerequisite for successful organ transplantation and the further treatment of organ recipients. I would like to address another important point: Can you tell us how many people received a donor organ in Switzerland last year and how many are waiting for one?
In 2023, 565 people in Switzerland received an organ (lung, heart, liver, kidney, pancreas, small intestine). However, at the end of 2023, 1391 people were still waiting for at least one organ, and 92 people died on the waiting list in 2023.
In the context of rising medical costs, the cost of transplants is naturally also being discussed in society. In your opinion, why is a transplant valuable for those affected, their environment and society despite the high costs?
Let me illustrate this with a kidney transplant. Compared to remaining on dialysis, the chances of survival for transplant patients are much higher. In addition, the quality of life after the transplant is completely different compared to life before the transplant, which was characterised by constantly recurring blood cleansing on the dialysis machine. Most transplant patients can therefore lead an almost normal life again. The costs of years of dialysis treatment borne by health insurance companies, and therefore ultimately by society, are massively higher than the costs of a transplant, including the associated medication for immune response suppression.
To conclude our discussion, let's take a look into the crystal ball. Are there any developments on the research horizon that will further improve the quality of life of people with a new organ?
In order to improve the quality of life of organ recipients, it is essential to select the organ that shows the closest match at the molecular level and therefore harbours the lowest possible risk of rejection. Structural analyses of the HLA molecules and improved bioinformatics tools make it possible to refine this matching even further.
The remaining risk of rejection can be reduced by a perfectly customised individual dose of immunosuppression. The individualisation of the dosage depends on the number of structural differences and the presentable peptides, which we can also determine as described.
I was extremely pleased to have this conversation with you about the importance of molecular correlations in organ transplantation. It became clear why the recipient body of a foreign organ does not accept it without objection. Your explanations also showed that molecular diagnostics is an essential part of the success story of transplantation. Thanks to the knowledge acquired over many years and the practices developed in diagnostics, it is becoming increasingly possible to allocate a suitable donor organ to the best possible recipient and to monitor the process after transplantation in the best possible way. Thank you very much for the interview.
Translated with DeepL
Gideon Hönger originally trained as a pharmacobiology laboratory technician and primary school teacher.
Since 2000, he has worked as a researcher and developer in the Laboratory for Transplantation Immunology and
Nephrology in the Department of Biomedicine at the University of Basel.
The main topics of many published studies are: Characterisation of donor-specific antibodies, alloimmunisation during pregnancy, HLA matching between organ donors and organ recipients at the epitope level.
In 2022 he completed his PhD at the University of Basel and in 2023 he obtained the European Diploma "Specialist Histocompatibility and Immunogenetics".
In addition to his research activities, he is co-head of the laboratory for HLA diagnostics and immunogenetics in the Laboratory Medicine Department of the University Hospital in Basel.